INTRODUCTION
Bone scans using technetium-labeled phosphate were found to detect bone fractures and metastasis in the early stages compared to general radiographs [1]. Therefore, bone scan is a commonly used modality for the evaluation of musculoskeletal lesions [2]. However, non-osseous radiopharmaceutical uptake on bone scans is often unexpected. Here, we report a case of diffuse splenic uptake of Tc-99m dicarboxypropane diphosphonate (DPD), which resembles a nuclear medicine spleen scan.
CASE PRESENTATION
A 47-year-old female presented with a history of alcoholic liver cirrhosis and splenomegaly underwent liver transplantation. The patient complain of lower backache and whole skeletal pain; a bone scan was performed to evaluate generalized osseous pain. A after 3h of intravenous injection oh 925 MBq Tc-99m DPD, whole-body images were recorded using a low-energy high-resolution collimator with a dual-head gamma camera (Symbia E, Siemens, USA)(Fig. 1).
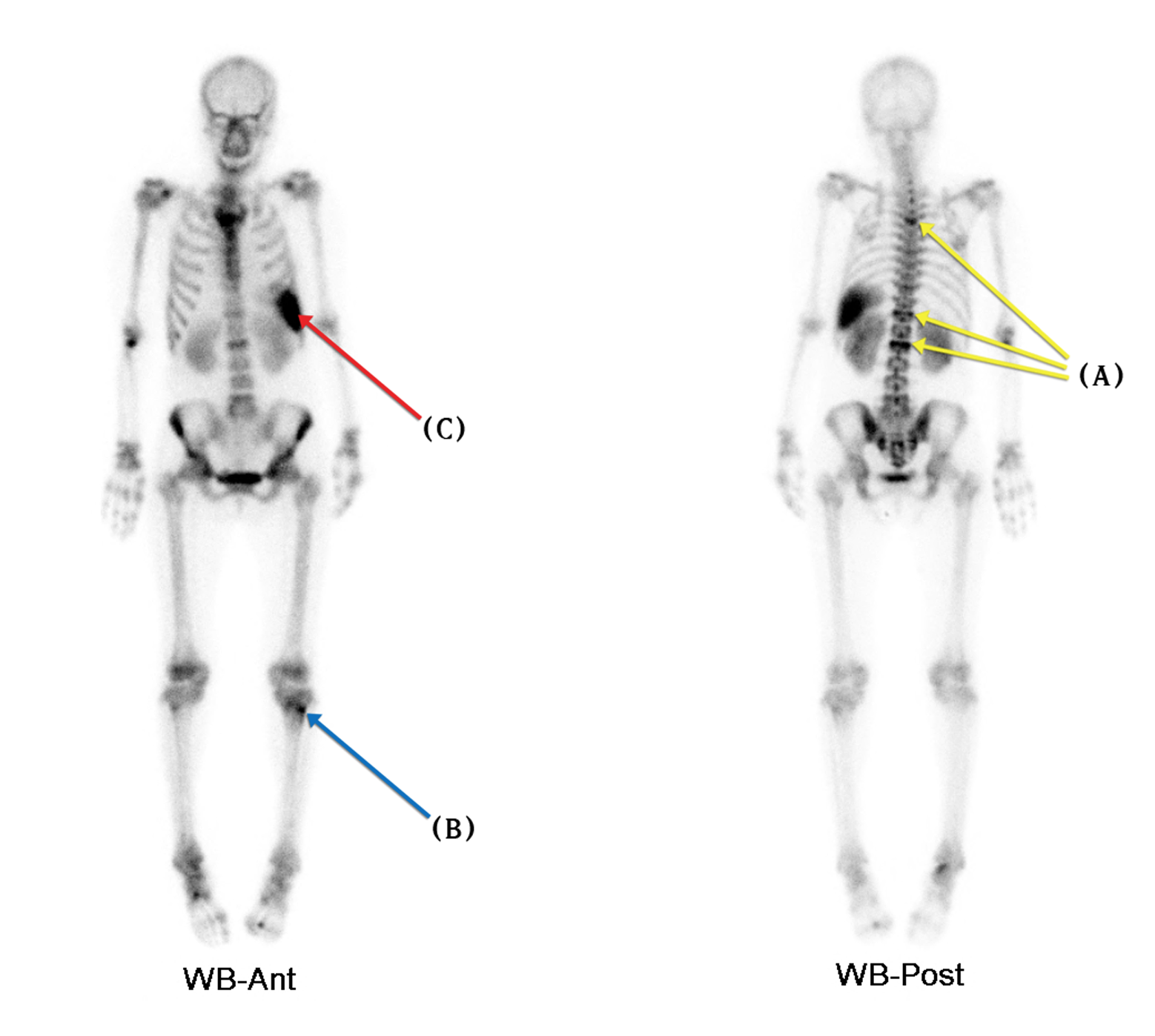
Fig. 1. Bone scan images show increased abnormal osseous uptake (A) on T4, T12, and L2 levels (compression fractures) and (B) left proximal tibia (suggestive traumatic bone lesion). Furthermore, they show increased (C) diffuse splenic uptake of radiopharmaceutical resembling nuclear medicine spleen scan.
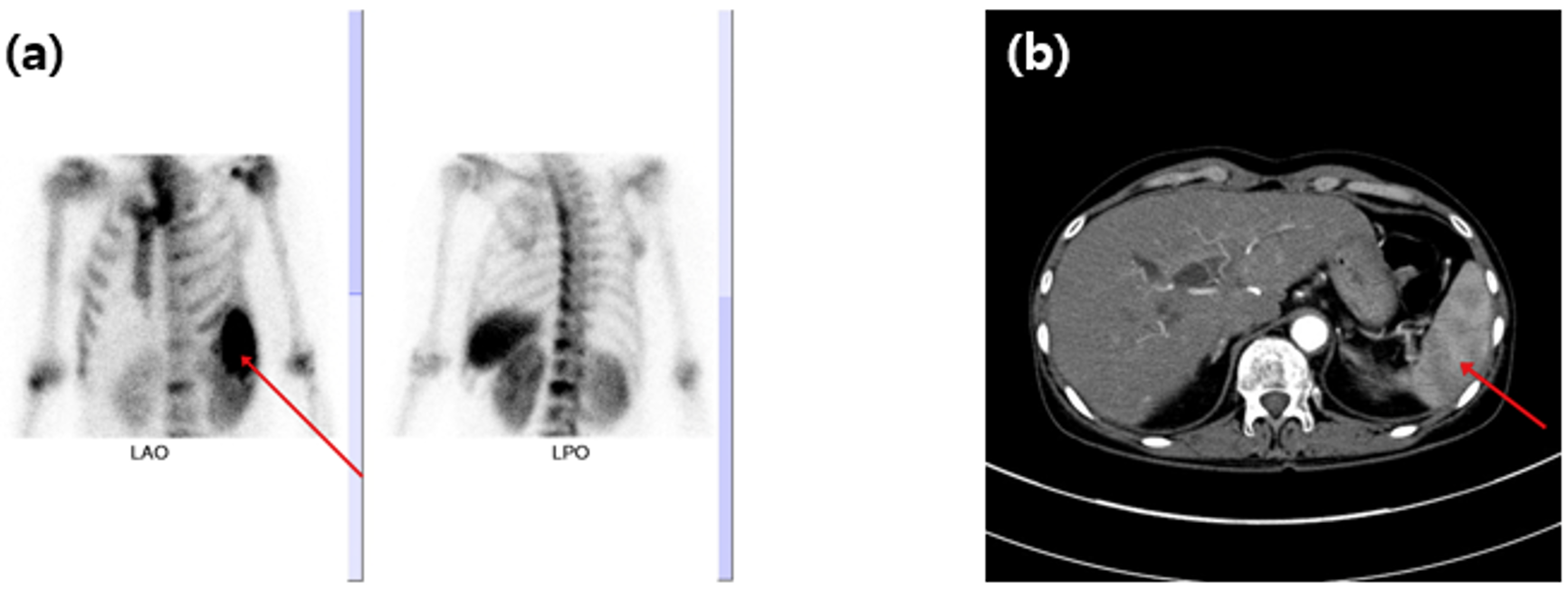
Bone scan images showed an increased diffuse splenic absorption of Tc-99m DPD (Fig. 2a). Contrast-enhanced computed tomography (CT) was performed. In this study, we performed contrast-enhanced CT, which revealed multiple poorly marginated, hypo-enhancing splenic lesions corresponding to infarction in the arterial and portal venous phases (Fig. 2b).
DISCUSSION
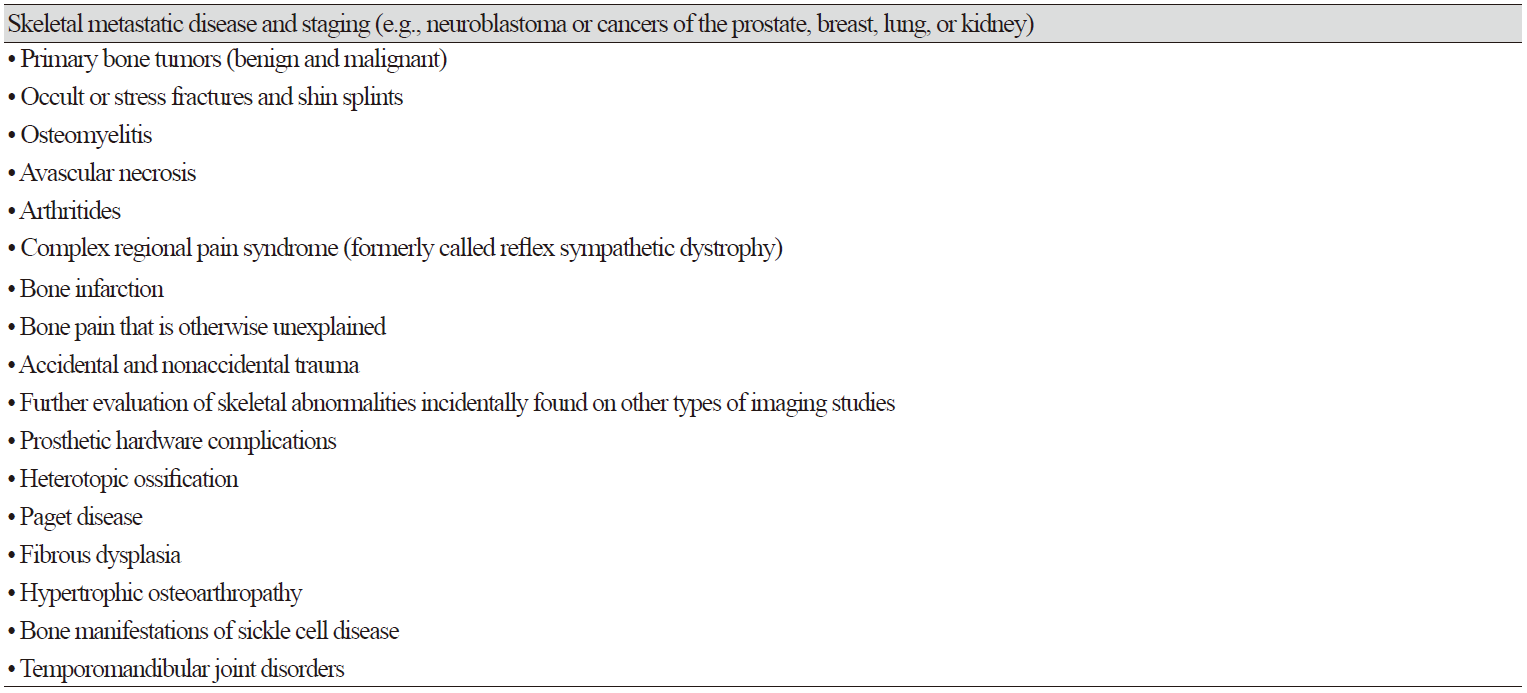
Bone scan images showed increased radiopharmaceutical absorption in lesions with increased osteoblastic activity. Table 1 lists common clinical indications for bone scans [1].
Unexpected radiopharmaceutical uptake in the spleen is occasionally observed during bone scans. The mechanism of splenic uptake of bone-seeking radiopharmaceuticals has been associated with the following finding [3-12]: residual radioactivity from a previous colloid scan, misadministration of radiocolloid, excessive aluminum ions from the generator, excessive serum aluminum, injection of radioiodinated contrast medium following bone agent injection, unknown metastatic calcification, hepatic necrosis, conditions of iron therapy, and compartmental sequestration. In this case, we can explain as splenic uptake of Tc-99m DPD was caused by multiple poorly marginated hypo-enhancing splenic lesions corresponding to the infarction.


